The US Food and Drug Administration (FDA) recently released a draft of their new guidance for
the development of anti-obesity medication (AOM) for weight reduction. Feedback will be
accepted until April 8. This guidance, replacing that published in 2007, attempts to incorporate
both changes to the AOM landscape and advances in our understanding of obesity as a
condition. We believe that this guidance will have implications for trial design and efficacy
benchmarks and for the competitive landscape of AOM.
In addition, although this guidance provides important clarity on a variety of points, we believe
that several outstanding questions remain unanswered. Here are our thoughts on several key
topics from the draft guidance.
Trial design
Inclusion criteria and endpoints
Both the FDA guidance and a recent commission from The Lancet Diabetes & Endocrinology,
which was published several weeks after the guidance and developed by 58 experts, highlight
body composition as a key component of obesity. The Lancet Commission characterizes
obesity as a condition of excess adiposity, and the guidance notes that AOM-induced weight
loss in patients with obesity should occur primarily from fat content reduction. A component of
this guideline is the FDA recommendation to measure body composition with dual-energy X-ray
absorptiometry (DXA) or an approved alterative in a representative subset of subjects (Note:
Waist circumference measurement is not an approved alternative).
It is interesting that the FDA guidance differs from The Lancet Commission with regard to use of
body mass index (BMI). The Lancet Commission recommends against using BMI as the sole
criterion for obesity, noting that it is an imperfect predictor of fat content. The FDA guidance
acknowledges limitations to the use of BMI as a proxy for body fat but does not view alternative
measurements of adiposity as superior to BMI; this is due to either limitations in accessibility or
challenges with reproducibility. The FDA guidance accordingly supports the standard inclusion
criterion of BMI ≥30 kg/m2 in AOM trials. The difference between the two groups’ stances may
reflect their different goals: an update to the theoretical framework of obesity by The Lancet
Commission, and an update to real-world practices by the FDA.
Sample size for safety data
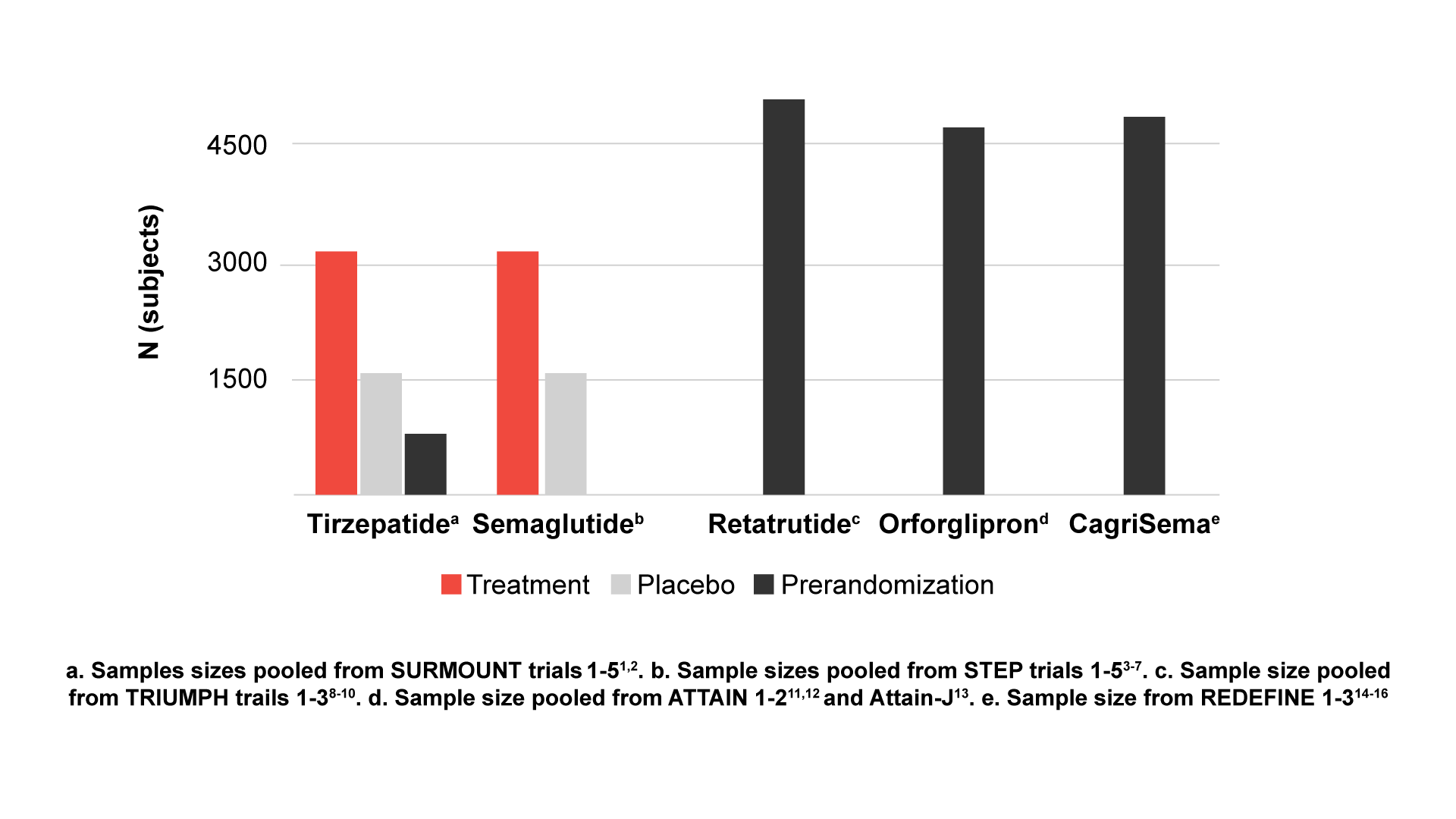
The FDA guidance recommends a sample size of 4500 participants to assess safety: 3000 for
the investigational drug, and 1500 for placebo. It is important to note that safety analysis can be
based on data from multiple trials. Recent phase 3 trials of tirzepatide1-2 and semaglutide3-7 have
each achieved this sample size when pooling subjects from their various phase 3 trials, and
ongoing trials for newer AOMs, such as retatrutide8-10 and orforglipron11-13 (Eli Lilly and
Company) and CagriSema14-16 (Novo Nordisk) are enrolling >4500 participants. We are curious
as to whether enrollment was scaled to ensure 3000 participants in the investigational drug
arms.
Patients with type 2 diabetes (T2D)
Phase 3 trials for tirzepatide and semaglutide were enriched for patients with T2D using drugs
for glycemic control, and there are reports of these drugs being prescribed for patients with
prediabetes (particularly during the delay between approvals for diabetes and obesity) and for
patients who meet neither disease’s criteria but could still benefit from treatment. The FDA
guidance builds on this approach by stating an expectation that trials be enriched for patients
with T2D who are using drugs for glycemic control, a requirement that will affect up-and-coming
AOMs in the developmental pipeline. It is interesting that the guidance also advises that an
indication for the delay of T2D onset will need to be supported by establishing the clinical
benefit(s) of the delay; delayed biochemical diagnosis of T2D alone would most likely not
suffice. Thus, although future AOM trials will need to be enriched for patients with T2D, approval
of these drugs for T2D treatment will be more challenging.
In addition, it is expected that once-weekly basal insulins for T2D treatment—molecules with
pharmacokinetic profiles that are fundamentally different from those of the daily versions—will
enter the US market in the coming years. Study sponsors will need to determine whether they
will differentiate between once-weekly and once-daily users in their analysis of T2D subgroups.
Efficacy
Historically, a mean percentage weight reduction that is at least 5% greater than that in the
control arm has been considered the threshold for clinical efficacy, and the FDA guidance now
specifies that this benchmark must be met for a drug to be considered effective for weight
reduction and maintenance in patients with obesity. It is common for drugs developed for other
conditions (eg, sodium-glucose cotransporter 2 inhibitors [SGLT-2is], selective serotonin
reuptake inhibitors [SSRIs]) to cause weight reduction that is statistically significant yet shy of
this mark, so this guidance ensures that drugs marketed as AOMs produce clinically meaningful
weight reduction.

cAMP = cyclic adenosine monophosphate; GIP = glucose-dependent insulinotropic polypeptide;
GLP-1 = glucagon-like peptide-1; RA = receptor agonist.
The FDA guidance also specifies that the 5% weight reduction must be maintained for at least 1
year, which addresses an important concern among healthcare professionals and patients
about the long-term efficacy of newer AOMs. It also appears to establish a need to both define
the maintenance dose itself and delineate key time points around goal attainment and
maintenance.
Competitive landscape
The FDA guidance also states that results will not be applied to drug classes as a whole and
that each drug will need its own trial, a distinction that could influence the ability to obtain certain
approvals. For example, insulins are a major class of weight-inducing drug, and the ownership
of most insulin forms by Lilly and Novo Nordisk gives them the edge of trialing their individual
insulins with their weight loss drugs. In addition, Lilly owns several psychotropic and
anticonvulsant drugs whose classes are associated with weight gain, which potentially confers
an advantage with approval of tirzepatide for treatment of the weight gain induced by these
same medications.
Conclusions
The AOM landscape continues to evolve rapidly. This FDA guidance helps address these
changes by codifying certain clinical trial practices and taking steps to ensure the real-world
efficacy of future AOMs. It will be interesting to see how the major pharmaceutical players
respond to the guidance and to compare the draft with its final version.
References
Please provide a valid e-mail address below to receive updates when new Blog content is available.
